Step-by-step plans without yoyo effect
A group of international scientists proposes a sustainable strategy in the Covid-19 pandemic


The coronavirus pandemic is in a critical phase. Tardy and inadequate measures have caused the winter wave to become protracted. Infection rates are now dropping and decisions about the next steps in the strategy are about to be taken. More infectious variants of the virus and the potentials for vaccination are playing a key role here. Another wave of infection due to a premature easing of restrictions should be avoided. Our proposal seeks to reconcile the Needs and desires of large parts of the population, as well as practical feasibility, with medical and epidemiological necessity. The main aim of this strategy, which aims at long-term sustainability, is to avoid a yo-yo effect, meaning the constant return of high infection rates caused by relaxing the rules too early. We seek to create a perspective for each citizen as well as for our society and the economy as a whole.
Against polarizing public debate
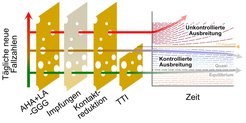
, the better the containment. The capacity of the TTI strategy, though, is limited when case numbers are high, because the actions of health authorities are slowed down and more infections go undetected for longer. A self-perpetuating pattern of virus spread takes hold. As the illustration shows, when case numbers are small, TTI is effective (blue, green) and numbers remain stable at a low level. When case numbers are high, we see a rise in infection numbers as well.")
A productive public debate about the strategy to fight the pandemic is immensely important. Unfortunately, this current debate is becoming increasingly polarized: People are typically identified as either advocates or opponents of lockdowns. There is too little differentiation based on the different and targeted measures. Our aim, as representatives of various disciplines, is to counteract this climate of polarization. Instead, we seek to bring together the various aspects that emerge from the trade-off between protecting health, meeting the needs of people and, not least, the social, psychological, cultural and economic collateral damage of protracted lockdown measures. In the future, we need to act in flexible ways that are targeted to specific contexts, rather than becoming entrenched in an either-or logic without any differentiation at all. And differentiated measures need differentiated criteria.
Choosing realistic and practicable goals
There are two poles in the debate about which target values and limit values are desirable and realistic: (1) a corridor with high incidences, without overburdening the health system, and (2) a swift and complete elimination of the virus.
If we go for a corridor at the capacity limit of the ICUs (pole 1), we could ease the restrictions temporarily. Before or – at the latest, when - the capacity limit is reached, however, the relaxations would have to be revoked. For case numbers to stabilize, harsher social restrictions are required when the incidence is high than when it is low. This is because the health authorities can do less to help containment when large numbers of people are becoming infected. To stay within a narrow corridor when case numbers are high, people's behavior has to be rigorously monitored. This is not realistic. Moreover, with this approach, we would need to accept that high numbers of people will contract the disease and die: More than 25 million people in Germany are between 50 and 75 years old. If they become infected by the coronavirus, their statistical probability of death is around 0.3 to 1 percent. In addition, the health system would become severely overstretched over a period of months, especially the ICUs. Neither should we ignore the long-term social, health and economic consequences of long COVID. We are unlikely to see an improvement of the situation due to vaccinations until the summertime. Finally, with this approach, there is no buffer for the containment of B.1.1.7 and other variants. The seasonal effect is not expected to balance this out either: If ot is at 20-30%, it may not even fully compensate the effect of B.1.1.7.
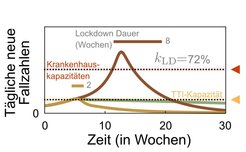
. Below the TTI capacity limit, far less contact limitation to stabilize the case numbers is needed, because health authorities play an effective part in the containment process. If the TTI capacity is exceeded, a fast lockdown can quickly reduce the case numbers. If too much time passes between xxxxx and xxxxx, a much longer lockdown is needed. TTI capacity limit depends on how well health authorities can work, how willing people are to cooperate and, of course, how much social contact they have. This limit, then, is not constant.")
Solutions at the second pole are aim to swiftly reach an incidence of zero. The crucial advantage, if this were to happen, is that the virus would not continue to spread. With just a few precautionary measures, we could lead a fairly normal life. In some regions, this target of zero target was reached last summer. At present, this would be difficult to maintain, since it would require extremely tightly knit testing at regional and national borders – which is neither possible nor desirable. In order to reach the absolute zero point from the current infection rate within just a few weeks, highly complex and rigid rules would have to be implemented, which would continue to severely limit public and social life.
These two extreme poles thus have considerable disadvantages. We are therefore proposing a strategy of local and differentiated containment that accepts that small local outbreaks can occur, but that seeks to keep the incidence consistently low (and reduce it further). The lower the incidence, the easier it is to control the outbreak. Health authorities can then isolate those having been in contact with infected people more quickly and break chains of infections. In this manner, it would be easier as well to prevent outbreaks in hospitals, care homes, shared accommodation and larger groups - because fewer undetected cases would slip through the cracks in the system. The same applies to large social gatherings, which can easily become superspreading events if the incidence is high. When the incidence is low, vulnerable groups are thus much better protected. And if low incidence is achieved within a large number of districts and states, we all benefit. Because the level at which infection rates will settle is proportionate to the rate at which the virus enters from outside.
From a sociological perspective, however, we must remember that low case numbers are not easy to achieve and maintain if there is no broad social consensus, and when it is also practically difficult for people to follow the rules. In this context, the following aspects need to be considered:
(1) Not everyone abides by the rules at all times. There are a number of reasons for this: First, when people are unhappy with the rules that are seen as ineffective or unfair, then motivation wanes. Second, although people's behavior is relatively to steer when they are in organized settings, they tend to become less alert when in more relaxed settings – during breaks in the workplace or in everyday situations. Third, the longer the crisis lasts, the more people struggle with social, psychological and financial problems and are no longer able to abide by many of the rules.
(2) Dropping or low case numbers increase the desire to see restrictions eased, and this makes it more difficult to abide by the rules in day-to-day life. This, in turns, negatively impacts infection rates the development of the case numbers. Any future strategy has to consider this mechanism.
(3) A liberal society cannot be completely controlled, neither when the incidence is low nor when it is high – and even if it could, this would not be desirable. It is because of this situation, not despite it, that we retain the ambitious goal of low incidence values. Contrary to what people often claim, this strategy does not deny them their freedom. The opposite is true: It aims to motivate people to work towards realistic goals, and ultimately gain more freedom that way.
But how do we implement it? Our overall strategy of local containment is based on a balancing of virological, epidemiological and sociological considerations. We combine the necessary reduction in the incidence and the R rate with deliberations about how to shape people's everyday behavior, and also with the consideration of the collateral damage caused by the pandemic. We seek to do this without playing these aspects off against one another.
The following aspects are key: For each measure introduced, it is necessary to clearly communicate the considerations and evidence that it is based upon; ideally, the data forming the basis of the evidence should also be made accessible to the public (and at the very least, to the scientific community). In addition to that, people must be provided with the resources they require to be able to comply with measures and rules. It is becoming increasingly important to be sensitive to inequalities and to mitigate them. This can be done, for example, with interim aid, government loans or stabilization programs that are not available only for companies but for private households as well. Direct support as well as social and therapeutic programs should be made available especially to people in precarious situations - as a matter of urgency. The medium and long-term aim must be to eliminate poverty – this is the only way to prevent hardship and stop society becoming even more polarized. And the only way to motivate large sections of the population and convince them of the measures.
Adaptive step-wise plans offer orientation
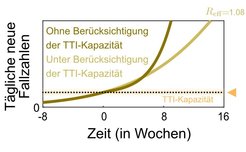
. If, however, the TTI capacity is exceeded, this rise is accelerated because more and more people carry the virus undetected. The numbers rise faster than exponentially (dark-colored line).")
We need well-considered step-wise plans that determine transparently which parts of public life can be opened, in which sequence – and on the basis of which considerations. The ultimate aim needs to be clear: Only when a stable and safe level of incidence has been reached, a targeted, intelligent and regionally specified easing of measures is possible. Our proposal is based, in the medium term, on a weekly incidence of 10 per 100,000 people, or even below this rate wherever this is possible. The numbers of 25, 35 or 50 are hard upper limits here, the objective being to achieve an adequate safety margin. If the incidence of 50 is exceeded, for example, harsh lockdown measures will need to be put in place as a matter of urgency. The faster and more effectively the incidence is reduced again after the limit values are exceeded, the quicker such a lockdown will be over.
The step-wise plan calls for representative infection rates, recorded from random tests throughout the population for example, regardless of whether a person is symptomatic or not. These data would also – broken down by region and age – make it much easier to evaluate the various containment strategies.
The step-wise plans currently under discussion are based primarily on incidence values. These values and the control mechanisms must be selected with caution to avoid the following three risk situations: (1) Restrictions are eased too early: This leads to another uncontrolled rise in case numbers and can forfeit the hard-earned successes. (2) Stagnation at incidence levels that are too high: The easing of restrictions slows the decline to such an extent that there is no further reduction of cases. If this happens in regions with high case numbers, restrictions need to be adjusted. Any further easing of restrictions becomes a distant possibility. (3) Inadequate response to rising case numbers: If the numbers rise, the measures are tightened as planned, but possibly not severely and quickly enough. The risk posed by new variants, which are more infectious or which bypass the immune system, has to be considered in all this. A staged plan, then, requires a strong mechanism that rigorously stops and reverses the rise in case numbers.
Test, monitor, vaccinate
Our society is a complex system in which many aspects interact. Measures to combat the pandemic, therefore, cannot be planned on the drawing board for the long-term; instead, we need to have an approach that perceives society as a learning system. As measures are developed, each and every step has to be clearly justified and communicated, evaluated and then adjusted as necessary. But this is only possible if we have the right data. The regular conducting of random tests in the population, which also includes people who are asymptomatic, is crucial here. The results of such tests can be used as the basis for assessing whether a specific combination of measures is effective or whether individual elements have to be adapted – for example when it transpires that certain activities affect outcomes in different ways then previously assumed.
This also applies for stage plans. The stage plans currently under discussion cover a number of areas in detail. The industrial sector and the job market, however, should also be explicitly included. Space, hygiene, mask + ventilation and app., avoiding closed rooms, groups, crowds and lively conversations side by side. Working from home or alternatively close testing regimes help to contain the pandemic.
All stages of easing restrictions should be accompanied testing. Rapid tests in particular can track down chains of infection at an early stage. For people to be tracked, traced and isolated before the contagion can spread, mandatory reporting of positive results should be implemented. Digital transformations within health authorities can be of assistance here. Without these follow-up measures, rapid tests do not develop their full potential. Access to rapid tests should not be a privilege, they should not be a financial burden on anyone. The number of rapid tests available is limited at present. Distribution should be controlled in a way that ensures there are enough tests available to protect the vulnerable, at the workplace, in schools, and so on. The principles for access to vaccines, protective equipment or masks ought to apply here too.
Vaccination programmes for the entire population are a promising route out of the pandemic. As well as improving the vaccination logistics, various vaccination schemes should be examined in clinical studies too.
Testing, technical measures, space, hygiene, mask + ventilation and app., avoiding closed rooms, groups, crowds and, as well as vaccination programs will help us to gradually contain the virus in the months ahead. Yet many questions remain unanswered. To what extent does vaccination reduce transmission? Which challenges will new virus variants pose? How long does immunity last, and how will the behavior of those who have received the vaccine change over the coming months? Until these questions have been answered and vaccination programs gives us some hope of an end to the pandemic, we consider the dynamically adapted strategy proposed here with an upper limit incidence rates as the best way out of the pandemic.
Authors and contributors
Sandra Ciesek, Institute for Med. Virology, University Hospital Frankfurt, Goethe University, Frankfurt
Thomas Czypionka, Institute for Higher Studies, Vienna, and London School of Economics
Armin Nassehi, Institute for Sociology, LMU Munich
Iris Pigeot, Leibniz Institute for Prevention Research and Epidemiology - BIPS, Bremen
Barbara Prainsack, Department of Political Science, University of Vienna; Department of Global Health & Social Medicine, King’s College London
Viola Priesemann, Max Planck Institute for Dynamics and Self-Organization, Göttingen
Anita Schöbel, Faculty of Mathematics, TU Kaiserslautern and the Fraunhofer Institute for Industrial Mathematics, Kaiserslautern
This text was published in a slightly abridged and amended form as a guest article in the German weekly newspaper Die Zeit on 17 February 2021.